

Our PDF editor allows you to fill out forms. You won't have to undertake much to update 24 petwatchi insurance claims documents. Simply keep up with all of these actions.
Step 1: To start with, select the orange "Get form now" button.
Step 2: Now, you're on the file editing page. You can add text, edit current details, highlight specific words or phrases, put crosses or checks, add images, sign the template, erase needless fields, etc.
Enter the information requested by the application to fill in the form.
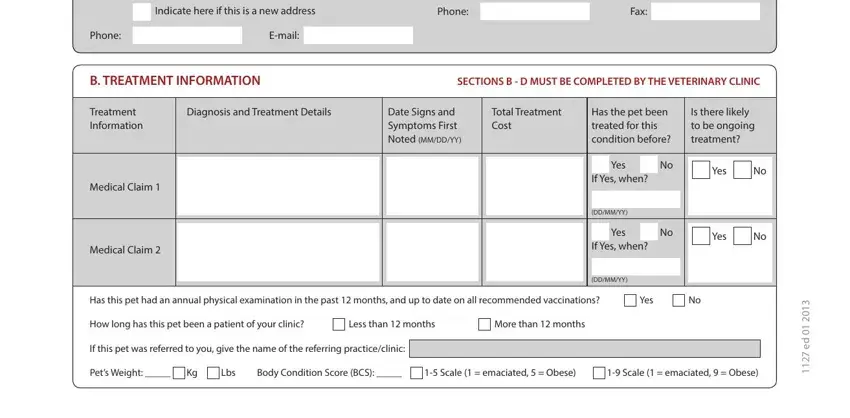
You have to write down the appropriate information in the Indicate here if this is a new, Phone, Fax, Phone, Email, B TREATMENT INFORMATION, SECTIONS B D MUST BE COMPLETED BY, Treatment Information, Diagnosis and Treatment Details, Date Signs and Symptoms First, Total Treatment Cost, Has the pet been treated for this, Is there likely to be ongoing, Medical Claim, and Medical Claim area.
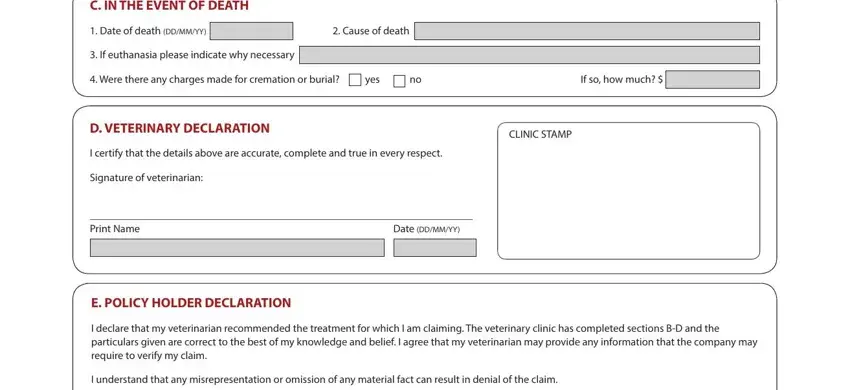
In the field dealing with C IN THE EVENT OF DEATH, Date of death DDMMYY, Cause of death, If euthanasia please indicate why, Were there any charges made for, yes, If so how much, D VETERINARY DECLARATION, CLINIC STAMP, I certify that the details above, Signature of veterinarian, Print Name, Date DDMMYY, E POLICY HOLDER DECLARATION, and I declare that my veterinarian, it's important to put in writing some required data.
In the field My total claim submitted is, Signed policy holder, Date DDMMYY, If you are claiming for the death, Applicable in Arizona For your, Applicable in Arkansas District Of, Any person who knowingly and with, Applicable in Indiana A person who, Applicable in Minnesota A person, Applicable in Nevada Pursuant to, Applicable in California For your, Applicable in Colorado It is, Applicable in New Hampshire Any, and Applicable in New York Any person, specify the rights and obligations of the sides.
Step 3: After you have selected the Done button, your form should be ready for upload to each gadget or email address you indicate.
Step 4: Come up with a minimum of a few copies of the document to remain away from any kind of possible concerns.
